Genetic radiation risks: a neglected topic in the low dose debate
Article information

Abstract
Objectives
To investigate the accuracy and scientific validity of the current very low risk factor for hereditary diseases in humans following exposures to ionizing radiation adopted by the United Nations Scientific Committee on the Effects of Atomic Radiation and the International Commission on Radiological Protection. The value is based on experiments on mice due to reportedly absent effects in the Japanese atomic bomb (Abomb) survivors.
Methods
To review the published evidence for heritable effects after ionising radiation exposures particularly, but not restricted to, populations exposed to contamination from the Chernobyl accident and from atmospheric nuclear test fallout. To make a compilation of findings about early deaths, congenital malformations, Down’s syndrome, cancer and other genetic effects observed in humans after the exposure of the parents. To also examine more closely the evidence from the Japanese A-bomb epidemiology and discuss its scientific validity.
Results
Nearly all types of hereditary defects were found at doses as low as one to 10 mSv. We discuss the clash between the current risk model and these observations on the basis of biological mechanism and assumptions about linear relationships between dose and effect in neonatal and foetal epidemiology. The evidence supports a dose response relationship which is non-linear and is either biphasic or supralinear (hogs-back) and largely either saturates or falls above 10 mSv.
Conclusions
We conclude that the current risk model for heritable effects of radiation is unsafe. The dose response relationship is non-linear with the greatest effects at the lowest doses. Using Chernobyl data we derive an excess relative risk for all malformations of 1.0 per 10 mSv cumulative dose. The safety of the Japanese A-bomb epidemiology is argued to be both scientifically and philosophically questionable owing to errors in the choice of control groups, omission of internal exposure effects and assumptions about linear dose response.
Introduction
The most serious effects of ionizing radiation–hereditary defects in the descendants of exposed parents–had been already detected in the 1920s by Herman Joseph Muller. He exposed fruit flies–drosophila–to X-rays and found malformations and other disorders in the following generations. He concluded from his investigations that low dose exposure, and therefore even natural background radiation, is mutagenic and there is no harmless dose range for heritable effects or for cancer induction. His work was honoured by the Nobel Prize for medicine in 1946. In the 1950s Muller warned about the effects on the human genetic pool caused by the production of low level radioactive contamination from atmospheric tests [1].
The International Commission on Radiological Protection (ICRP) recently decreased its risk estimate for heritable damage in 2007 [2,3]. Its Detriment Adjusted Nominal Risk Coefficient for radiation heritable effects in an exposed population was reduced from the previous 1990 value of 1.3% Sv-1 to 0.2% Sv-1 a greater than 6-fold reduction. The ICRP approach is based on a linear relation between dose and end-point, measured as heritable disease at or before birth. Evidence and arguments which we will present suggest that this linear assumption is invalid and that the ICRP value is unsafe when applied to the chronic low dose internal exposure range.
The belief that heritable consequences of radiation were negligible followed from studies of the Japanese survivors of the atomic bomb (A-bomb) explosions in Hiroshima and Nagasaki in 1945. The American-Japanese Institute in Hiroshima, Atomic Bomb Casualty Commission (ABCC), did not apparently find mutations in the descendants of the survivors. Therefore the ICRP derive its current risk figure from experiments in mice. The result corresponds to the evaluation by the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR committee) [4].
We will show that the current model for genetic effects of exposure is unsound and we present a more realistic one based on data. We will begin by pointing to some serious problems with the ABCC studies of genetic effects in the A-bomb survivors. These may be classed under four Error Types.
Type 1. The dose response problem. For genetic damage, increasing dose will not linearly increase effects since at high doses there will be sterility or fetal loss [5].
Type 2. The external/internal problem. The dose of interest is the energy delivered to the germ cells and their precursors. This may be much higher for internal radionuclides with affinity for DNA (strontium-90 [Sr-90], barium-140, uranium) [6].
Type 3. The philosophical method problem. If data is interpreted though a particular scientific model, evidence which cannot fit the model will be ignored, dismissed or invisible [7,8].
Type 4. Bias in the analysis of or presentation of data from the ABCC results. There have been a number of serious criticisms of the ABCC and later studies of cancer effects. The genetic studies were criticised by De Bellefeuille [9] who demonstrated the existence of significant genetic effects including sex-ratio and malformations which had been “lost” through the choice of analysis. However, De Bellefeuille’s observations were ignored by the risk agencies. The issue will be returned to in the discussion section.
Together these raise major doubts over the belief, expressed in ICRP103, Appendix B.2.01 [2], that “Radiation induced heritable disease has not been demonstrated in human populations.”
Effects in populations exposed to Chernobyl fallout are excluded by the official committees, which claim that doses are too low to generate statistically observable increases (the philosophical method problem: Error Type 3). This, however, is certainly wrong, because we know from many studies of chromosome aberrations, either that the doses calculated by UNSCEAR are much too low or that there is an enhanced radiobiological effectiveness (RBE) in the type of internal exposures or chronic delivery received by the Chernobyl groups. In other words, the biological or genetic damage from unit internal dose e.g., from a radioactive atom bound to DNA is far greater than for the same dose delivered externally. This is Error Type 2: internal/external problem. The doses upon which the ICRP risks are based, either from humans or mice, are external doses. There are significant issues regarding the equivalence for causing genetic damage of internal and external dose calculations [6]. Internal exposure to uranium by inhalation, for example, has been associated with significantly high genotoxicity resulting in anomalously high excess levels of chromosome damage and birth defects in a number of different groups [10]. Uranium binds to DNA, a fact that has been known since the 1960s [11-13]. Other group II calcium mimics and DNA seekers include the nuclide Sr-90 which causes significant genetic effects [14-17]. All epidemiological studies of radiation and health which define risk factors have been subject of this Error Type 2: external/internal problem, and have generally also defined risk in terms of cumulative integrated equivalent dose, and so real effects have been ignored or dismissed, the Error Type 3: philosophical problem.
Findings in Children Born After the Chernobyl Accident and in Kazakhstan
We previously published findings about fetal deaths, perinatal mortality and congenital malformations (CM) after Chernobyl [18]. Table 1 shows results for CM after Chernobyl. These appeared not only in the area of the exploded reactor but also in Turkey, Bulgaria, Croatia, and Germany. Our criteria for inclusion of this evidence was originally to present only observations which disagreed with the current ICRP/UNSCEAR paradigm but following questions by a reviewer we include discussion of one of the few studies with contemporary data which claims to have shown that there were no measurable heritable effects [19].

Increase of congenital malformations after exposure by the Chernobyl accident
The EUROCAT Europe-wide Study
The study of Dolk and Nichols [19] is widely cited as evidence for no effect. The authors examined Down’s syndrome, neural tube defects (NTD), microcephaly, hydrocephaly, anopthalmos and congenital cataract in 16 EUROCAT registers. There were 231401 births in the areas in 1986. The 16 registries were divided into three groups of high (200 to 800 μSv), medium (97 to 190 μSv) and low (29 to 55 μSv). Three comparison cohort periods were defined as E (conception May 1986), T (conception May 1986 to April 1987 contains E), and C (control: conception May 1987 to April 1989). Authors concluded “no evidence of a generalised detectable increase in the prevalence of congenital anomalies in the first month or first year following Chernobyl.” But the choice of the cohort periods for a study of “heritable effects” is interesting. On the basis of whole body monitoring results, genetic damage to the germ cells from internal exposures will have continued well into the control period C and damage will have been cumulative [44]. We have reanalysed their data for combined NTD hydrocephaly, microcephaly and anopthalmia in all their exposure groups using their periods. A test of T vs. C cohorts showed a significant effect with odds ratio (OR) of 1.20 (95% confidence interval [CI], 1.02 to 1.4; p=0.014). This was apparent in the test of E vs. C though the numbers were smaller. However, there was no increasing monotonic relation between assumed “dose” category and effect and this clearly influenced the authors’ conclusions. This is the common response to the finding of high risks at low doses and represents a good example of the Error Type 1 referred to above. It appears that the results actually show an increased risk if we combine all the exposure levels.
Chernobyl Effects in Belarus
Belarus received most contamination from Chernobyl. A central registry for CM existed from 1979 and rates of CM before and after the Chernobyl accident could thus be compared. A number of studies are listed in Table 1. Comparison of legal abortuses in 1982 to 1985 and 1987 to 1994 showed combined CM increases of 81%, 49%, and 43% in regions of high (>555 kBq/m2), medium (>37 kBq/m2), and low (<37 kBq/m2) contamination, the effect being significant at the 0.05 level in all three [22]. The genetic origin is confirmed in those anomalies which are combined with a recognized mutation that is not present in either of the parents [18].
A study [23] confirmed the CM excess in the Strict Registration of Malformations System finding 86% increase in 1987 to 1996 vs. 1982 to 1985 (high contamination) and 59% (control regions) (p<0.05). The same authors reported significant excess chromosome aberrations of dicentric and centric rings rates of 0.39±0.09% (n=91) in Gomel and Mogilev (>555 kBq/m2) compared with a control region of Minsk, Grodno and Novopolotsk (<37 kBq/m2) (n=118; CM=0.09±0.04) [23].
To 2004 there was no decrease in these rates [45]. The authors think these effects are genetically induced because it is not plausible that doses in pregnant females rose in the period of decreasing environmental contamination and decreasing food contamination after the accident. A Belarussian-Israeli group [46] found the following increased polygenetic disease rates in children of Chernobyl- exposed parents: hematological diseases (6-fold), endocrine diseases (2-fold), diseases of digestive organs (1.7-fold).
A 1994 study compared Gomel (high exposure) with Vitebsk (presumed low exposure) for mortality in children zero to four finding absolute CM rates of 4.1% vs. 3%, respectively [24]. Savchenko [25] writing for the United Nations reported frequency of CM in regions of Gomel between 1982 to 1985 and 1987 to 1989 ranging from 170% in Dobrush to 680% in Chechersk.
Petrova et al. [27] compared two high and two low contaminated regions of Belarus for a number of indicators of pregnancy outcome and child health. For CM, before and after Chernobyl increases for all CM were: Gomel 150%>Mogilev 130%>Brest 120%>Vitebsk 110%, the rank of their contamination levels. Kulakov et al. [26] examined 688 pregnancies and 7000 births in Chechersky (Gomel, Belarus) and Polessky (Kiev, Ukraine). Sharp reductions in birth rates in both regions after Chernobyl were ascribed partly to abortions. High perinatal mortality was ascribed partly to congenital malformations. Incidence increased by a factor of two following the accident for congenital heart disease, esophageal atresia, anencephaly, hydrocephaly and multiple malformations. Total number of neonatal disorders increased in Polessky (Ukraine) from 1983 to 1985 to 1986 to 1990 from 6.81 to 21.32 (313%) and in Chechersky from 5.15 to 10.49 [26].
Chernobyl Effects in Ukraine
The studies by Wertelecki and colleagues [29,30] were valuable for quantifying the effects. The Pripyat region of Ukraine on the border of Belarus was significantly contaminated. Populations are dependent on local produce. Internal contamination was quantified for two groups, a high and lower dose group by whole body monitoring for caesium-137 (Cs-137). In addition, local produce was analysed for both Cs-137 and the DNA seeking Sr-90. The Sr-90/Cs-137 ratio was between 0.5 and two, so Sr-90 (with its DNA affinity and anomalous RBE) represented a significant internal exposure.
Other Reports of Chernobyl Effects on Birth Defects; Soviet Nuclear Test Site
Down´s syndrome as a certain genetic effect increased in several contaminated European countries [18,48]. An example is shown in Figure 1. In West Berlin, which was a kind of closed island at that time, the geneticist Sperling registered a sharp and significant increase in cases exactly nine months after the accident, also in Belarus [49]. UNSCEAR [4,20] dismissed these findings (and similar reports from Scotland and Sweden) on the basis that the doses were “below background.” The EUROCAT combined registry study [19] did not find an increase in Down’s syndrome, neither in the authors’ analysis nor in our reanalysis. Other evidence is presented in Table 1 of increased CM rates after Chernobyl in Germany, Turkey, Croatia and Bulgaria [21,32-37,50].
Congenital effects were found near the former Soviet nuclear test site in Kazakhstan near Semipalatinsk. Sviatova et al. [51] studied CM in three generations of inhabitants, investigating births between 1967 and 1997. They found significantly increased rates of CM combined, including Down’s syndrome, microcephaly and multiple malformations in the same individual.
Hereditary Effects in Children of Exposed Mothers
If a population is exposed, genetic effects will occur in the gonads of mothers as well as of fathers. A German investigation of occupationally exposed females showed a 3.2-fold significant increase in congenital abnormalities, including malformations, in offspring [52]. The authors interpret the effect as generated in utero but do not prove such a connection. In our opinion, this appears to be improbable given the short sensitive phase in pregnancy and the ban on pregnant females working in high risk environments.
The findings confirm early results in the Department of Medical Genetics of Montreal Children’s Hospital where the genetic effects of diagnostic X-rays were investigated [53]. The author observed the offspring of mothers who had been treated in childhood for congenital hip dysplasia since 1925 and were X-rayed for several times in the pelvic region. The ovarian dose was estimated to lie between 60 mSv to 200 mSv. In 201 living births of these females there were 15 individuals with severe malformations and other congenital distortions or Down’s syndrome and 11 cases with other abnormalities (all congenital abnormalities 12.9%) while the control group showed less than half of this rate. The latter was chosen from a large group of descendants where the parents were unexposed siblings of the study group.
Taken together with other evidence from sex-ratio (discussed below) these studies indicate that hereditary effects exist in the children of exposed mothers.
Findings in the Descendants of Occupationally Exposed Men Including Nuclear Test Veterans
Congenital Malformations
Studies in children of exposed men where the mothers were not exposed will show definite hereditary effects. A compilation of results for CM in offspring of exposed fathers is given in Table 2.

The anomalies seen in the descendants of Chernobyl liquidators (Nos. 5-7) also indicate unexpectedly high radiation sensitivity.
Three studies of nuclear test veterans have shown large increases in congenital effects in children and one study has found similar levels of congenital conditions in the grandchildren (Nos. 8-10). The British carried out nuclear weapon tests and activities in Australia (Maralinga) and Christmas Island in the Pacific between 1952 and 1967. More than 20000 young national servicemen and other military personnel were stationed at the test sites. The sites were contaminated with fission fallout and nanoparticles of uranium and plutonium from the weapons, tritium and carbon-14. Urquhart [61] analysed data in children from 1147 veteran families. Two hundred and thirty-three out of them had illnesses or defects (cancer, malformations, mental retardation) that could have a genetic origin: one in five families. They registered a 7:1 rate of abnormal children conceived before the tests vs. those conceived after the tests.
Two further studies of the offspring of a group of veterans have been published. Roff [62] carried out a questionnaire study of members of the British Nuclear Test Veteran Association (BNTVA) and reported excess rates of cardiovascular disorders, spina bifida, hydrocephalus and hip deformities. Busby and de Messieres [63] examined a different sample of the BNTVA, employed controls and compared with the European EUROCAT rates. Based on 605 veteran children and 749 grandchildren compared with 311 control children and 408 control grandchildren there were significant excess levels of miscarriages, stillbirths, infant mortality and congenital illnesses in the veterans’ children relative both to control children and expected numbers. There were 105 miscarriages in veteran’s wives compared with 18 in controls (OR, 2.75; 95% CI, 1.56 to 4.91; p<0.001). There were 16 stillbirths; three in controls (OR, 2.70; 95% CI, 0.73 to 11.72; p=0.13). Perinatal mortality OR was 4.3 (95% CI, 1.22 to 17.9; p=0.01) on 25 deaths in veteran children. Fifty-seven veteran children had congenital conditions vs. three control children (OR, 9.77; 95% CI, 2.92 to 39.3; p<0.001) these rates being also about eight times those expected on the basis of UK EUROCAT data for 1980 to 2000. For grandchildren similar levels of congenital illness were reported with 46 veteran grandchildren compared with three controls (OR, 8.35; 95% CI, 2.48 to 33.8; p<0.001).
Cancer and Leukemia
In 1984, an exceptionally high level of leukaemia cases in children and juveniles was reported in Seascale, near the nuclear reprocessing plant in Sellafield in Cumbria, UK. The authors explained this as a hereditary effect, because the fathers of the patients had worked in the plant [64]. The authorities argued that the doses were too low. The effect, however, had been described in principle already in experimental studies [65], and also after X-ray diagnostic exposures (Table 3). A significant number of other child leukemia and cancer studies have been carried out and are listed in Table 3.
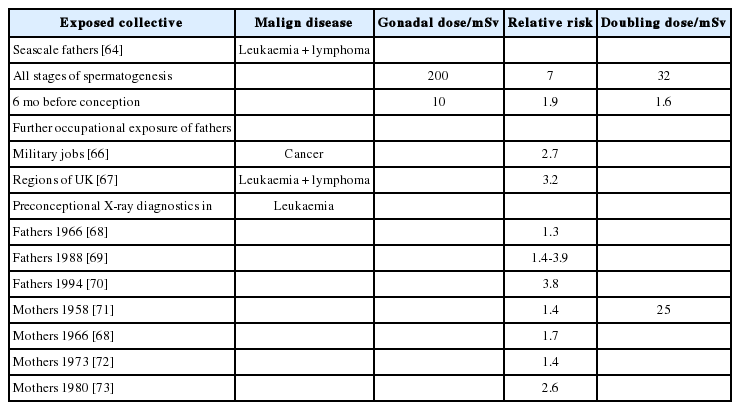
Cancer in children after preconceptional low-dose exposure of parents
The research of Hicks et al. [66] concerned exposed servicemen (Table 3). McKinney et al. [67] found a 3.2-fold increase in leukaemia and lymphomas in children of occupationally exposed men in three British regions in a case-control study.
Sex-ratio and X-linked Lethal Factors
Normally, it is not possible to study how many inseminated oocytes (zygotes) will be aborted after irradiation of the gonadal cells in humans. But it is observed that males who were exposed have fewer daughters than sons i.e., the male/female sex-ratio increases with dose.
Gene mutations may be responsible for the death of the zygote and will also occur in the sex chromosomes where they will predominantly affect the greater X-chromosome which can only be transmitted to a daughter. A dominant lethal factor will then lead to the death of the female zygote. Recessive lethal factors in the X-chromosome are much more frequent than dominant ones [74]. They affect only female births.
An impressive result was obtained in workers of the British nuclear fuel reprocessing plant at Sellafield in West Cumbria [75]. The county sex-ratio was 1055 boys/1000 girls, the normal value. For the children of fathers employed at Sellafield the ratio was 1094. For those with recorded doses greater than 10 mSv in the 90 days preconception period it was 1396, significant at the p<0.01 level. A similar effect was detected in cardiologists, who undertook interventional angiographic procedures involving X-ray exposures [76].
Scherb and Voigt studied different groups of inhabitants in a variety of countries after the Chernobyl accident for hereditary effects and found radiation-induced foetal deaths and early mortality, Down’s syndrome and alterations of the birth sex-ratio. They examined nuclear tests above ground which affected US inhabitants, Chernobyl emissions in Europe, and those living near German and Swiss nuclear plants. Results showed significant reduction in the female birth rate in all these [77,78].
The ABCC studies overall involve all the types of research error listed in the introduction, which we believe is the explanation for the failure to see excess heritable damage. The main problem was choice of controls. The sex-ratio studies were abandoned due to seemingly anomalous effects. De Bellefeuille [9] re-examined the issue in 1961 and found that results were biased by employing sex-ratios of children of parents who had both been exposed. Any effects, being in opposite directions, would therefore cancel out; his re-analysis based on children with only one exposed parent showed a clear effect in the expected direction. Padmanabhan [79] recently re-examined the issue using the original controls (abandoned by ABCC). Using the two not in city (NIC) groups Padmanabhan showed significant sex-ratio effects in the expected directions.
Sex-ratio is a very relevant parameter. It shows that genetic alterations are induced in the germ cells of males by very low doses, and it proves to be a sensitive indicator for exposures of the population.
Atmospheric Weapons test Fallout
The most significant global incident in terms of human exposure has been the atmospheric nuclear testing fallout which peaked between 1959 and 1963. It was this testing which worried Muller [1]. The tests increased the rates of neonatal and infant mortality in the US and the UK [80,81]. An interesting insight comes from a Canadian study of CM during the fallout period. le Vann [82] was concerned to examine the link between congenital malformation and the use of the drug thalidomide. He found that in Alberta there was no relation between the use of thalidomide and congenital birth outcomes but noted a strong association with precipitation; areas with high radioactive fallout had high levels of birth defects. Whilst we are not alleging that thalidomide does not have teratogenic effects, since many females in the le Vann study who never took any drugs gave birth to the typical “thalidomide spectrum” babies it seems that exposure to the fallout may have, as Muller [1] feared, have caused an effect. Ignoring this and the infant mortality findings involved a Error Type 3.
Genetic vs. Genomic, Mendelian vs. In Utero
We have not distinguished between Mendelian genetic effects involving the transfer of specific gene mutations to the offspring and effects consequent upon the operation of genomic instability, whereby the offspring inherit a tendency to apparently increase rates of all mutation above the normal rate for that population [83]. For the purposes of the arguments relating to radiation risk of harmful heritable conditions in the first generation such a discussion is unnecessary but needs to be revisited if multi-generational effects are being discussed. The question of germ cell damage in parents vs. in utero damage to development, though important, seems to us to be beside the point. All these CM effects are caused by mutation of DNA whether in the parental germ cells and precursors or from implantation to birth. Our aim is to assess the genetic risk based on observations. However, from the sex-ratio results it would seem that parental exposure is a dominant cause of radiation induced CM.
How Is It That the ICRP Risk Coefficient Is Wrong?
A reviewer asked us to address this question and to provide a brief account of biological mechanism. We begin with mechanism. The ICRP risk model is based on two big ideas: absorbeddose, which is average energy per unit mass of tissue, and the linear no threshold (LNT) response. For internal exposure to substances like Sr-90 and uranium, which both have high affinity for DNA, the concept of dose is meaningless [loc.cit. 6,10]. For CM as an outcome, it is also clear that the LNT model is unsustainable [5], because as the “dose” is increased from zero there are many blocks to the successful journey from germ cell to infant, the CM end point. Biological plausibility would predict an increase in damage and thus CM at very low dose, followed by a drop in CM due to failure to implant, early miscarriage, abortion. This would result in a saturation or “hogs-back” dose response in the lowest dose region. Only the survivors would make it to be registered as CM. The dose response would look like that in Figure 2 where A is the initial outcome and B is where the foetus dies or there is no implantation. The region C would relate to in utero effects later in gestation. There would be a fall in birth rate associated with region B and C; there usually is. You can see this effect most clearly in the EUROCAT studies where relative risk rises and then falls as dose increases [19]. It is perfectly clear in many other studies. It is clear in in analysis of infant leukemia after Chernobyl in 5 countries shown in Figure 3 [84] and the study of cleft palate in Bavaria [38,39] analysed by Korblein [40].

Regions of interest in a theoretically predicted dose response relation (see text and ECRR 2010). Exactly this dose response is seen in infant leukemia rates after Chernobyl in Greece, Germany (three dose regions) Wales, Scotland and Belarus [84]. From Busby C. Aspects of DNA damage from internal radionuclides; 2013 [6]. aQ is the background cancer rate in the population at background radiation levels, the position where the graph starts.
What Is the Correct Risk Coefficient?
The Chernobyl studies presented in Table 1 may be used to obtain an approximate risk factor for all CM in those exposed to fission spectrum radionuclides as assessed by Cs-137 area contamination. We can employ the data from Wertelecki et al. [30] on internal contamination to assess doses from Cs-137 and Sr- 90. The excess relative risk (ERR) for all CM follows a “hogsback” shaped response and is about 0.5 per mSv at 1 mSv saturating at between 0.1 to 0.2 per mSv at 10 mSv based on cumulative dose as assessed by ICRP models using Cs-137 area contamination as a basis of calculations. This means that the background rate will double or treble up to 10 mSv exposure and thereafter flatten out or fall. But it also results in a 50% excess risk at doses as low as 1 mSv. This ERR and dose response model accommodates all the observational data from Chernobyl and also elsewhere. We must make it clear that this model is for mixed internal and external exposure to fission product contamination doses as employed by UN agencies and may not necessarily apply to pure external exposures (e.g., X-rays, gamma- rays). However, it should be noted that Stewart’s finding of a 40% excess risk of childhood leukemia after a 10 mSv obstetric X-ray dose [71] is comparable with what is found at these higher doses in this review.
Conclusion
Genetically induced malformations, cancers, and numerous other health effects in the children of populations who were exposed to low doses of ionizing radiation have been unequivocally demonstrated in scientific investigations. Using data from Chernobyl effects we find a new ERR for CM of 0.5 per mSv at 1 mSv falling to 0.1 per mSv at 10 mSv exposure and thereafter remaining roughly constant. This is for mixed fission products as defined though external exposure to Cs-137. Results show that current radiation risk models fail to predict or explain the many observations and should be abandoned. Further research and analysis of previous data is suggested, but prior assumptions of linear dose response, assumptions that internal exposures can be modelled using external risk factors, that chronic and acute exposures give comparable risks and finally dependence on interpretations of the high dose ABCC studies are all seen to be unsafe procedures.
Acknowledgements
We are grateful to Marvin Resnikoff and Rick Haaker for running the Microshield program for dose rates over contaminated areas.
Notes
The authors have no conflicts of interest associated with material presented in this paper.