INTRODUCTION
Atopic dermatitis, asthma, and allergic rhinitis are chronic diseases that are common in infants [1,2], and the allergic disease prevalence in Korea has been consistently increasing [3, 4]. The increase in allergic diseases has been an important public health problem in society because these diseases cause sleep disorders, impede growth, disrupt education [5,6], and significantly increase the socioeconomic burden by lowering the quality of life for the family [7,8].
Because the prevalence of allergic diseases is closely related to age and dependent on the type of allergic disease, the symptoms manifest at different ages [9]. In foreign studies evaluating the prevalence of allergic diseases in children and infants, the rate of atopic dermatitis was highest in children under 5 years of age, asthma symptoms were highest in children between 2 and 9 years of age, and allergic rhinitis was highest in those between 6 and 11 years of age [10]. While research has been conducted in Korea to evaluate allergic diseases in children, few studies have evaluated the prevalence of allergic diseases before infancy. According to the International Study of Asthma and Allergies in Childhood (ISAAC) conducted by Oh et al. [4] the prevalence of 'atopic dermatitis symptoms during the past 12 months' for the year 2000 was 10.7% in children between 6 and 12 years of age and 6.1% in those between 12 and 15 years of age, whereas the prevalence of 'atopic dermatitis symptoms during the past 12 months' for the year 2003 was highest in 5-year-old children, with a prevalence rate of 21.1%. The second highest prevalence rate was found in elementary and middle school students. After investigating the prevalence of allergic diseases throughout Korea among elementary school students, i.e., 3rd, 4th, and 5th grade students, using 'symptoms of the past 12 months' as a standard, Suh et al. [11] determined the prevalence of atopic dermatitis, asthma, and allergic rhinitis to be 15.3%, 4.8%, and 32.9%, respectively. Kwon et al. [12] analyzed elementary school students in the region of Seoul in 2008 and determined the prevalence of asthma symptoms to be 5.5%, whereas the prevalence of asthma treatment had been 2.7% during the previous 12 months.
There have been several epidemiological studies evaluating the prevalence of allergic diseases in Korea, but due to variations in the diseases studied, the starting point of the investigations, and the age of the subjects, we were unable to perform systematic comparisons to determine changes in prevalence according to age. Nonetheless, because allergic diseases have a number of symptoms that are expressed differently according to age, the effective management of allergic symptoms requires a better understanding of the prevalence of these diseases during infancy.
Because the existence of subjects with multiple allergic reactions (i.e., multiple allergic diseases) is not rare, a patient with one allergic disease has an increased probability of developing another allergic disease [13]. For example, atopic dermatitis is an important risk factor in the development of additional allergic reactions [14]. In research performed in Beijing on subjects between 0 and 14 years of age, the percentage of children with asthma who were also suffering from dermatitis was 45.2%, the percentage of children with asthma who were also suffering from allergic rhinitis was 49.5%, and the percentage of children with both asthma and dermatitis was 23.1% [10]. Allergic diseases may manifest themselves by demonstrating aspects of multiple allergic diseases where many symptoms appear together, but there are very few studies on multiple allergic diseases in Korea.
The purpose of the present study was to determine the prevalence of individual allergic diseases and of multiple allergic diseases based on child subjects between the ages of 0 and 13 years.
MATERIALS AND METHODS
I. Subjects and Design
This study enrolled 38,201 children between 0 and 13 years of age from 34 elementary schools and 136 children's daycare centers to participate in the 'Seoul Atopy Friendly School' survey from May to October 2010. Elementary schools from 19 out of 25 districts (excluding Nowon, Mapo, Yangchun, Dongjak, and Seocho) and children's daycare centers from 21 districts (excluding Jongno, Gangbuk, Dobong, and Gangnam) participated in the 'Seoul Atopy Friendly School' survey.
II. Questionnaire
The questionnaire gathered basic personal data and information related to the prevalence of allergic diseases for each subject. Because the clinical manifestations of allergic diseases vary, prevalence can be demonstrated differently depending on how the disease is defined. However, it is possible to assess and compare the prevalence of allergic diseases across the world using the ISAAC questionnaire [15]. The prevalence indices for atopic dermatitis, asthma, and allergic rhinitis used were 'symptoms in the past 12 months' and 'experience of treatment in the past 12 months'. For atopic dermatitis, a question such as, 'Has your child had an itchy rash at any time in the past 12 months?' was asked. If the response was 'Yes', it was counted toward 'the prevalence of atopic dermatitis symptom in the past 12 months'. A question such as, 'Has your child been treated for eczema in the past 12 months (congenital fever or atopic dermatitis)?' was then asked. If the response was 'Yes', it was counted toward 'the experience of treatment for atopic dermatitis in the past 12 months'. For asthma, a question such as, 'Has your child had wheezing or whistling in the chest in the past 12 months?' was asked. If the response was 'Yes', it was counted toward 'the prevalence of asthma symptom in the past 12 months'. A question such as, 'Has your child ever been diagnosed and treated for asthma in the past 12 months?' was then asked. If the response was 'Yes', it was counted toward 'the experience of treatment for asthma in the past 12 months'. For allergic rhinitis, a question such as, 'In the past 12 months, have you had a problem with sneezing or a runny or blocked nose when you did not have a cold or the flu?' was asked. If the response was 'Yes', it was counted toward 'the prevalence of allergic rhinitis symptom in the past 12 months'. A question such as, 'Has your child ever been treated for allergic rhinitis in the past 12 months?' was asked. If the response was 'Yes', it was counted toward 'the experience of treatment for allergic rhinitis in the past 12 months'.
III. Statistical Analysis
All of the statistical data were calculated using STATA version 10.0 (StataCorp, College Station, TX, USA). The general characteristics of the subjects are presented as the means±standard deviations for continuous variables and as frequencies for categorical variables. A cross-analysis of the subject's age and allergic disease was implemented. To calculate a trend in the prevalence of allergic diseases according to age, a general linear model was implemented. In all the analyses, a p-value < 0.05 was regarded as statistically significant.
RESULTS
I. General Characteristics
Twenty-five districts in the capital, Seoul, were divided according to their location, and 5 adjacent districts were combined for the analysis. The distribution of the subjects is presented in Table 1. For the first area (Jongno, Jung, Yongsan, Seongdong, and Gwangjin), 7,015 children from 10 elementary schools and 22 children's daycare centers participated in the study. The second area (Dongdaemun, Jungnang, Seongbuk, Gangbuk, and Dobong) included 6,010 children from 5 elementary schools and 29 children's daycare centers. For the third area (Nowon, Eunpyeong, Seodaemun, Mapo, and Yangcheon), 4,242 children from 4 elementary schools and 33 children's daycare centers participated in the study. The fourth area (Gangseo, Guro, Geimcheon, Yeongdeungpo, and Dongjak) included 4,512 children from 4 elementary schools and 33 children's daycare centers. Finally, the fifth area (Gwanak, Seocho, Gangnam, Songpa, and Gangdong) included 9,422 children from 11 elementary schools and 32 children's daycare centers. A total of 31,361 subjects (82.1%) responded to the questionnaire, but only the data from the 31,201 subjects without missing information were analyzed. Out of a total of 170 Atopy Friendly Schools, 34 elementary schools (20.0%), 136 children's daycare centers (80.0%), 24,240 elementary school students (77.7%), and 6,961 toddlers (22.3%) were studied. Out of the 31,201 subjects, 51.1% were male, and the ages ranged from 0 to 13 years (Table 2). Out of all of the subjects, the children aged 10 to 13 years made up the majority (38.2%). Children aged 7 to 9 years comprised 35.3% of the total study population, children aged 4 to 6 years comprised 16.9%, and children aged 0 to 3 years comprised 9.6%.
II. Symptom Prevalence of Allergic Diseases and Experience of Treatment
In Table 3, 'symptom prevalence of atopic dermatitis, asthma and allergic rhinitis in the past 12 months' and 'experience of treatment for atopic diseases in the past 12 months' by age and gender are reported. The table shows that the prevalence of atopic dermatitis symptoms in the past 12 months was 16.6% on average (19.3%, 19.7%, 16.7%, and 14.5% for children 0 to 3 years of age, 4 to 6 years of age, 7 to 9 years of age, and 10 to 13 years of age, respectively). The prevalence in male children was highest for children between 0 and 3 years of age (21.1%), and the prevalence in female children was highest for those between 4 and 6 years of age (20.9%). As the children became older, the prevalence showed a tendency to decrease (p for trend <0.001). The treatment frequency for atopic dermatitis in the past 12 months was 13.3%, and it was highest for children between 0 and 3 years of age (18.8%).
The prevalence of asthma symptoms in the past 12 months was 7.6% on average (16.5%, 9.8%, 6.5%, and 5.4% for 0- to 3-year-old, 4- to 6-year-old, 7- to 9-year-old, and 10- to 13-year-old children, respectively). In all the age groups, the prevalence was higher in male children than in female children. The treatment frequency for asthma in the past 12 months was 3.4%. In children 0 to 3 years of age, the treatment frequency was 4.1% (4.8% in males and 3.3% in females).
The prevalence of allergic rhinitis symptoms in the past 12 months was 36.5% on average (28.5%, 38.0%, 38.5%, and 35.9% for children 0 to 3 years of age, 4 to 6 years of age, 7 to 9 years of age, and 10 to 13 years of age, respectively) and was highest in male children between 7 and 9 years of age (42.8%). In all the age groups, the prevalence in male children was higher than in female children. The treatment frequency for allergic rhinitis in the past 12 months was 22.4%. The treatment frequency was highest in children between 7 and 9 years of age (25.2%). In all the age groups, the treatment frequency was higher in male children than in female children.
'Symptom prevalence' and 'treatment frequency' differ in that some subjects who have symptoms are not medically treated. The differences between these two groups were 3.3% for atopic dermatitis, 4.2% for asthma, and 14.1% for allergic rhinitis. When comparing the differences according to gender, there was a higher proportion of male children compared to female children who were not medically treated despite the appearance of symptoms. For atopic dermatitis, the differences between these two groups were 3.0% for male children and 2.6% for female children. For asthma, the differences between symptom prevalence and treatment frequency were 4.7% for male children and 3.4% for female children. For allergic rhinitis, these differences were 14.5% for male children and 12.2% for female children.
III. Prevalence of Comorbid Allergic Diseases
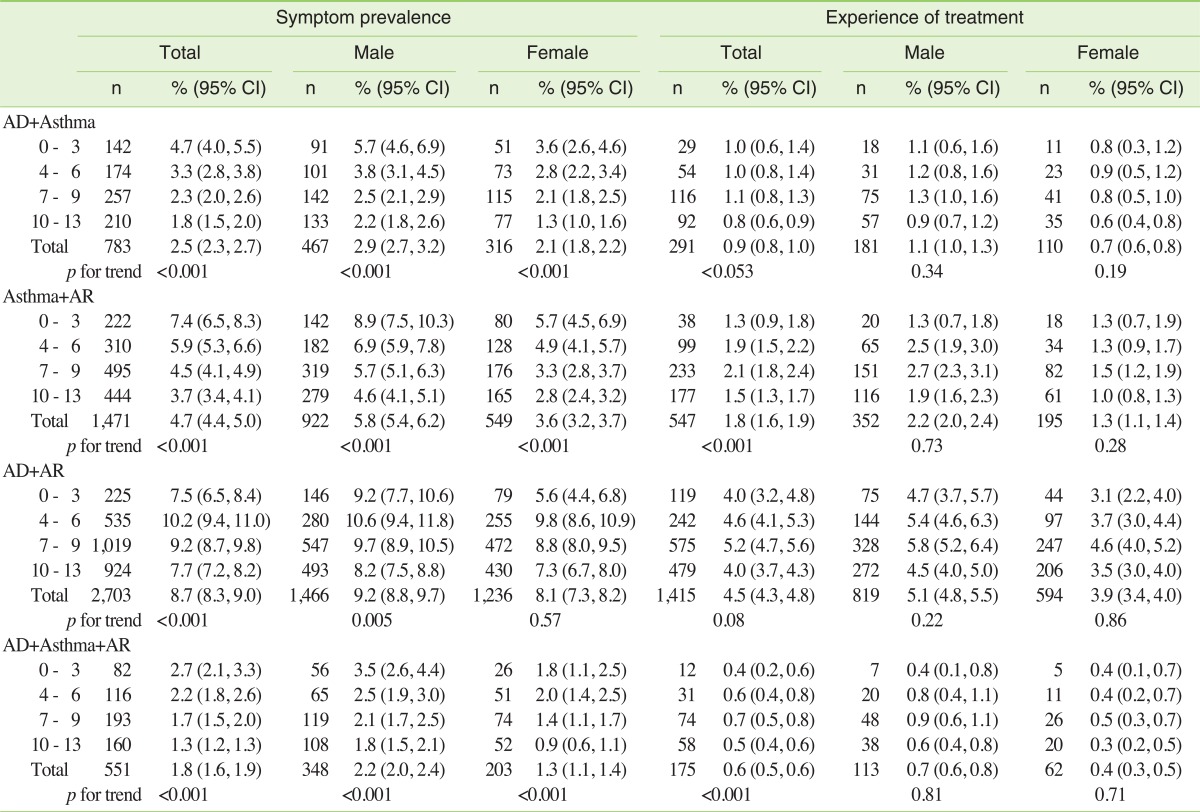
In Table 4, the prevalence of comorbid allergic diseases is presented. In instances where the patient had both atopic dermatitis and asthma, the prevalence was 2.5% and was highest in children between 0 and 3 years of age, with a prevalence of 4.7% (5.7% in male children and 3.6% in female children). By gender, 2.9% of male children and 2.1% of female children had symptoms of both atopic dermatitis and asthma. The treatment frequency for both atopic dermatitis and asthma was 0.9%.
The prevalence of asthma and comorbid allergic rhinitis was 4.7%. The prevalence in male children was 5.8%, while the prevalence in female children was 3.6%. The prevalence of these diseases was highest in children between 0 and 3 years of age at 7.4% (8.9% in male children and 5.7% in female children). The treatment frequency for both asthma and allergic rhinitis was 1.8%.
In situations where the patient had symptoms of both atopic dermatitis and allergic rhinitis, the prevalence of symptoms in the past 12 months was 8.7%. The prevalence was highest in the 4- to 6-year-old age group, with a prevalence of 10.2% (10.6% in male children and 9.8% in female children). The treatment frequency for both atopic dermatitis and allergic rhinitis was 4.5%. The proportion was highest in the 7- to 9-year-old age group, with a prevalence of 5.2% (5.8% in male children and 4.6% in female children).
The prevalence of comorbid symptoms of atopic dermatitis, asthma, and allergic rhinitis was 1.8% (highest in 0- to 3-year-old children, with a prevalence of 2.7%). The highest prevalence rates observed were 3.5% in 0- to 3-year-old male children and 2.0% in 4- to 6-year-old female children. The treatment frequency for atopic dermatitis, asthma, and allergic rhinitis was 0.6%.
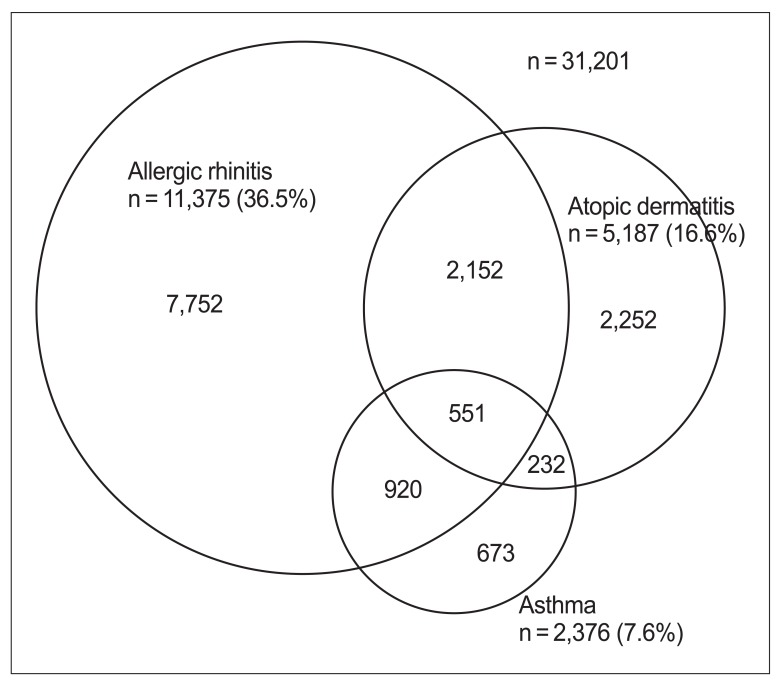
Using 'symptoms in the past 12 months' as the standard, only 2,252 subjects (43.4%) experienced atopic dermatitis symptoms, while the other subjects (56.6%) suffered from asthma, allergic rhinitis or had both diseases with comorbid atopic dermatitis (Figure 1). Of 2,376 subjects, 673 (28.3%) had symptoms of asthma without an accompanying disease, and 7,752 out of 11,375 subjects (68.1%) had symptoms of allergic rhinitis without other allergic disease.
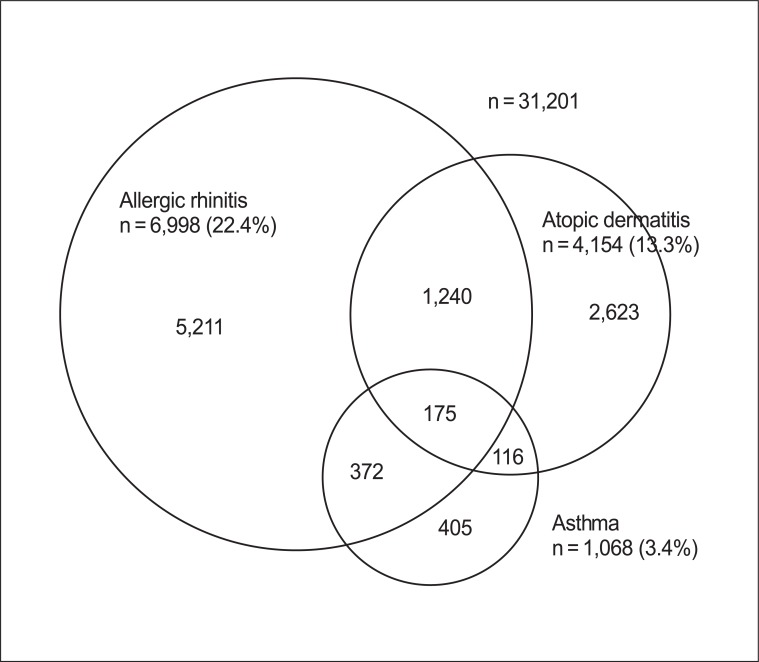
Using 'experience of treatment in the past 12 months' as the standard, 2,623 subjects (63.1%) received treatment for atopic dermatitis alone without any accompanying treatments (Figure 2). The remaining subjects (36.9%) received treatment for asthma or allergic rhinitis or for both diseases in addition to treatment for atopic dermatitis. Similarly, 405 out of 1,086 subjects (37.9%) received treatment for asthma only, and 5,211 out of 6,988 subjects (78.4%) were treated for allergic rhinitis only.
DISCUSSION
This study aimed to analyze the prevalence of individual and comorbid allergic diseases in children aged 0 to 13 years who participated in a Seoul Atopy Friendly School survey. Using 'symptoms in the past 12 months' as the standard, the prevalence of atopic dermatitis was consistently high in children less than 6 years of age, while the prevalence of asthma and allergic rhinitis was highest in children 0 to 6 years of age and in children greater than 4 years old, respectively. Male children had a higher prevalence of atopic dermatitis, asthma, and allergic rhinitis than female children. The prevalence of patients with both atopic dermatitis and asthma, asthma and allergic rhinitis, or atopic dermatitis and allergic rhinitis was 2.5%, 4.7%, and 8.7%, respectively. The prevalence of having all three diseases was 1.8%. The percentage of subjects who experienced at least one of the many symptoms associated with at least one of the three diseases in the past 12 months was 46.6%. For atopic dermatitis and asthma, the prevalence of symptoms tended to decrease as age increased.
In Korea, several studies have been performed to evaluate the prevalence of allergic diseases using the ISAAC questionnaire [4,11,12]. Based on the data obtained from 3rd, 4th, and 5th grade elementary school students, we compared the results from previous studies [11] to our study. The results of this comparison are as follows: the prevalence of atopic dermatitis symptoms in the past 12 months in previous studies and in our study was 15.3% vs. 16.7%, respectively; the experience of treatment for atopic dermatitis in the past 12 months was 13.7% vs. 13.1%, respectively; the prevalence of asthma symptoms in the past 12 months was 4.8% vs. 6.3%, respectively; the experience of treatment for asthma in the past 12 months was 2.5% vs. 3.3%, respectively; the prevalence of allergic rhinitis symptoms in the past 12 months was 32.9% vs. 40.4%, respectively; and the experience of treatment for allergic rhinitis in the past 12 months was 21.3% vs. 26.1%, respectively. For every condition evaluated, except for 'the experience of treatment for atopic dermatitis in the past 12 months,'the prevalence observed in our study was higher than in previous studies. This result may be because the previous studies conducted by Suh et al. [11] targeted all the provinces throughout the country, including the industrial complex regions, whereas our research evaluated only subjects living in Seoul. For example, there were significant differences in the prevalence of atopic dermatitis symptoms according to the area of residence (15.4% in the city, 13.6% in the province, 11.4% in the countryside, and 15.9% in the industrial complex)
It is well-known that the prevalence of atopic dermatitis, asthma, and allergic rhinitis present with different characteristics according to age, but few studies have investigated the prevalence of allergic diseases throughout childhood. When comparing this study to the study performed in Beijing that studied children 0 to 14 years of age using the ISAAC questionnaire, the rate of subjects with 'symptoms in the past 12 months' with atopic dermatitis were high among children 0 to 4 years of age [10]. However, as the subjects aged, the prevalence showed a tendency to decrease significantly. In our study, the prevalence of atopic dermatitis was high among children 0 to 3 years of age and 4 to 6 years of age, but the prevalence decreased as the subjects aged. The prevalence of 'symptoms in the past 12 months' among children with asthma in Beijing was highest for children between 2 and 9 years of age, and the prevalence of 'symptoms in the past 12 months' among the subjects with asthma in this study was highest for those between 0 and 6 years of age. Our study demonstrated a high prevalence of asthma, especially for children between 1 and 3 years of age; however, because wheezing and whistling sounds are common at that age, it may have been difficult to differentiate these sounds from asthma symptom sounds [16]. This phenomenon, however, was not observed in the Beijing study, and the authors suggested that this was due to the difference in the way people answered the questions. In the Beijing study, the prevalence of allergic rhinitis was highest in children between 4 and 11 years of age [10], while in our study, the prevalence increased as age increased. The above results confirm the progression of allergies (such as atopic dermatitis, asthma, and allergic rhinitis) in which the symptoms appear either simultaneously or sequentially as time progresses [17]. To reduce the progression of allergic diseases, management policies that consider the differences in the prevalence of the disease according to age must be established.
Our study demonstrated that, with the exception of two or three different age groups, asthma and rhinitis have a higher prevalence among male children than female children. These results support the results obtained from previous studies [10,11,18,19]. A previous study suggested that the cycling of sex hormones according to gender and age may influence the prevalence of asthma in males more so than in females before puberty, but this phenomenon reversed as the subjects went through puberty [20]. In a cohort study in Finland, the prevalence of asthma was higher in male children than in female children, but between the ages of 22 and 32 years, the prevalence was the same for both genders [21]. In an animal experiment, the female sex hormone progesterone was shown to have the greatest effect on the prevalence of asthma according to gender, and an even higher effect was observed when the subject smoked [22].
Allergic diseases such as atopic dermatitis, asthma, and allergic rhinitis often appear sequentially according to age, though many symptoms occasionally appear at the same time [23]. This indicates that asthma and allergic rhinitis share a similar pathological mechanism and that clinical expression occurs on the upper or lower side of the respiratory organs [24,25].
Based on British research, the prevalence of multiple allergic diseases is 11% for children between the ages of 2 and 15 years, 10% for individuals between the ages of 16 and 44 years, and 5% for people over the age of 45. The prevalence observed in subjects between 2 and 15 years of age who were diagnosed with asthma, dermatitis, and rhinitis was 2% [7]. From Britain's primary care database, which contains information on the prevalence of 2 or more allergic diseases between 0 and 90 years of age, the prevalence was highest among those between 10 and 14 years of age. After this age, the prevalence decreases as age increases [26]. However, this study analyzed only the number of allergic diseases and did not take into account the effects caused by different types of diseases.
In addition to the reasons suggested in previous studies with respect to the comorbidity of allergic disease, other possible explanations include a fillagrin mutation (one of the factors that cause atopic dermatitis and asthma) or the occurrence of food allergies [27]. Fillagrin is a substrate protein located underneath the stratum corneum that protects the skin from the environment. Genetic mutations of fillagrin are known to increase the occurrence of allergization, atopic dermatitis, allergic rhinitis, and asthma in a person with a skin disease [28]. In addition, a modification of fillagrin leads to a weakening of the skin wall, which, at a young age, presents as dermatitis and then later becomes a risk factor for asthma [29,30].
The strength of this research is that it is the first study conducted in Korea to examine the prevalence of individual allergic diseases and multiple allergic diseases in subjects between 0 and 13 years of age. Previous studies have only investigated elementary school aged children or a few age groups at different ages. However, this research simultaneously investigated children between 0 and 13 years of age. Furthermore, previous studies have only examined the prevalence of individual allergic diseases, but because there has been no research on children between 0 and 6 years of age, it has been difficult to explain the progression of allergic diseases in young children.
An additional strength of this research is that the use of the ISAAC questionnaire has made it possible to compare the results of this study to the prevalence of allergic diseases in other countries. In the ISAAC study, a phase III investigation was performed with 5 to 10 year intervals after the initial investigation. According to the results from 143 centers, 60 countries, and 385,853 children between 6 and 7 years of age who participated in the phase III ISAAC research, the prevalence of atopic dermatitis symptoms in the previous 12 months ranged from 0.9% to 22.6%. In our study, the prevalence for the same age group and the same symptoms was 17.9%, a prevalence that ranked 5th out of 60 countries [15]. The prevalence of asthma symptoms in the past 12 months for children between 6 and 7 years of age in our study was 8.1%. Compared to the prevalence of asthma for the same age group according to the ISAAC study, which included subjects from 66 centers in 34 countries, our study ranked 26th out of 37 countries, indicating that the prevalence of asthma was relatively low in our study [31]. The prevalence of allergic rhinitis symptoms in the past 12 months in our study was 38.9%, which was much higher than the global average of 20.7%. Out of 66 centers, only 4 centers reported a prevalence of allergic rhinitis symptoms in the past 12 months higher than 30%: Fukuoka (Japan), Taipei (Taiwan), Bangkok (Thailand), and Costa Rica.
The weakness of this study is that disease severity, the period of disease contraction, the family history of disease, and lifestyle were not analyzed. Furthermore, there may be some problems with respect to representativeness because the procedure used to enroll institutions did not adhere to the probability sampling process. However, because all of the 25 districts in Seoul participated in this study, and the elementary schools and children's daycare centers that participated were equally distributed throughout the 5 larger areas, it is believed that the prevalence obtained from this study may reflect the prevalence throughout Seoul. The prevalence obtained from this study tended to be higher than that obtained in previous studies. This may be due to increases in the prevalence of allergic diseases. However, it is predicted that environment and lifestyle could have contributed to this increase, and therefore, in the future, this possibility must be investigated.
The results of this study demonstrate the prevalence of allergic diseases in children from Seoul. This study investigated not only individual allergic diseases but also comorbid allergic diseases that manifest at similar times according to age groups. This information is pertinent for the development of a treatment regimen for allergic diseases.