Introduction
According to the World Health Organization (WHO), consuming tobacco is one of the most important global public health threats, causing more than seven million deaths annually [1]. In this regard, target 3.a of the Sustainable Development Goals (SDG3.a) aims to reinforce the implementation of the World Health Organization Framework Convention on Tobacco Control (FCTC) in all countries [2–6]. This is consistent with other items of the SDG3 including SDG3.4 [2,6,7]. According to Gunter et al. [8] in 2018, approximately 38.2% of Korean adult males and 5.9% of Korean adult women were smokers. This indicates that the total smoking rate among adult Koreans in 2018 was around 22%. To improve the Koreans’ public health situation on the road to achieving SDG3, promoting smoking cessation based on realistic tobacco exposure risk assessment is essential. To achieve this, understanding accurate smoking behavior is necessary for social approaches to the development of effective smoking cessation programs.
There are several options to measure an individual’s smoking behavior, including self-report surveys and using smoking topography instruments [9]. Despite the higher costs, topography measurement instruments are being used to determine smoking behaviors in several studies [10–13]. Investigation of smoking habits through a self-report survey is an easy way to investigate smoking habits, which have considerable potential as an indicator of smoking intensity for evaluation of population-based smoking habits [14]. In particular, studies of Yang et al. [15] and Shahab et al. [14] indicated that results of self-report puff behavior variables are associated with the level of cotinine in urine and saliva, which are biomarkers of exposure to tobacco smoke.
Nevertheless, it is essential to investigate the reliability of the smoking habits survey by comparing it to the machine-determined smoking topography. In 2008, Shahab et al. [14] showed that for a group of 118 smokers from Australia, Canada, the United Kingdom, and the United States, the correlation between puff counts per cigarette and inter-puff intervals measured through self-report surveys with the ones measured using the CReSSmicro instrument are weak but statistically significant. On the other hand, results of a similar but more recent study conducted by Pulcu [16] in 2016 on 110 smokers in the United Kingdom indicate that smokers may underestimate the puff counts per cigarette. This underestimation was evaluated to be very significant because it could reduce susceptibility to the incidence of respiratory diseases.
Despite the importance of this matter, there is a limited number of studies on the evaluation of smoking behaviors of Korean smokers [7,10,11,15]. Most of these studies investigate the machine-determined smoking topography of Korean smokers with the biomarker of exposure to tobacco smoke. Therefore, fewer studies are designed to investigate the scalability and reliability of measuring smoking behaviors through self-report surveys compared to machine-determined ad-libitum daily smoking topography. Accordingly, this study aims to investigate the smoking habits of a group of Korean adults through a self-report survey, measure the daily ad-libitum smoking topography of the participants, and compare the results of these two investigations and measure their correlations.
Materials and Methods
Recruiting subject and the self-report smoking habit survey
Recruitment of subjects was conducted as described by Yang et al. [7]. Macromill Embrain Co. (Seoul, Rep. of Korea) recruited 100 smokers through a nationwide online invitation. Applicants who smoke any type of tobacco products except ordinary filtered cigarettes, pregnant women, and those who reported diagnosis of any mental or physical disorders, including smoking-related respiratory diseases were excluded. Immediately after the recruitment and before conducting the smoking topography experiment, the smoking habit survey we designed was conducted online by Macromill Embrsain Co. The main questions, aimed at identifying the smoking habits of smokers, are summarized in Table 1.
The raw results of the survey were compared with the associated ones measured using the portable CReSS Pocket device. The estimation of smoked cigarettes per day in the survey was done using equation 1. In this equation, CPDSurvery is the estimated amount of smoked cigarettes per day, CPDWeekdays and CPDWeekends refer to the number of smoked cigarettes during weekdays and weekends, respectively, as self-reported by the smoker in the survey.
To investigate the smoking volume through the self-report smoking habit survey, a rank order scaling question is used to extract details on the smoke inhalation depth. The scale was ranged from 1 (no inhalation) to 10 (deep inhalation down to the lung), and the bigger number may indicate higher inhalation of smoking volume. The survey also included the Fagerström Test for Nicotine Dependence (FTND) [17]. The FTND includes items such as time to first cigarette (TTFCFTND) and number of daily smoked cigarettes (CPDFTND). The FTND score was used to evaluate the nicotine dependency of the participants and compare its association with smoking behavior variables measured by the self-report smoking habit survey and the smoking topography measurement device. The evaluation of nicotine dependency as very low, low, medium, high, and very high was done by considering the FTND score range of 0–2, 3–4, 5, 6–7, and 8–10, respectively [7,17].
Smoking topography experiments
The smoking topography experiments were conducted as described by Yang et al. [7] under careful consideration of the COVID-19 infection prevention protocols. Recruited participants were invited to visit the Institute for Environmental Research at Yonsei University College of Medicine, located in Seoul, Republic of Korea. The objectives and procedure of the study, data analysis, and privacy protection policies were comprehensively explained to all subjects. They subsequently signed a letter of consent and were compensated. A unique identification code was assigned to each participant. The Institutional Review Board (IRB) of the Severance Hospital of the Yonsei University Health System approved the study design. For each participant, smoking topography variables, including the number of recorded smoked cigarettes (CPDDevice), puff counts (PCDevice), puff time (PT), inter-puff interval (IPI), and total daily smoking volume (TSVDevice) were measured using a set of portable CReSS Pocket devices made by Borgwaldt KC GmbH (Hamburg, Germany). For each participant, the experiment is conducted for two days. On the first day, the participant gets a topography measurement device and learns how to use it. Each participant is asked to use the device for ad-libitum smoke of all cigarettes for 24 hours and return it on the second day. The participants were also asked to carefully record the time they wake up on the second day and report it when they return the device. For any device returned on the second day, raw recorded data downloaded from it and broken puff records, with puff duration <0.05s, were excluded. For each participant, total smoking time was estimated using equation 2 [7,16]. The time to first cigarette (TTFCDevice) is calculated by considering the differences between the reported wake-up time and the device-recorded time of the first cigarette after the reported time.
Statistical analysis
Information provided by the self-report smoking habit survey is based on the knowledge of the smoker about himself. In contrast, using topography measurement devices may affect how they smoke, especially during the first few smoking events [18]. Accordingly, to conduct a more realistic comparison between the parameters of the self-report smoking habit survey and machine-determined smoking topography as well as minimize the effect of outlier data on further analysis, we considered the study conducted by De Jesus et al. [18]. For each participant, we calculated the 95% confidence interval (CI) of the measured variables, except CPDDevice and TTFCDevice. We then excluded the data out of the 95% CI and proceeded with statistical analysis. As for PCSurvey and TSTSurvey, the median of the ranges in multiple choices was considered as the indicator number for further statistical analysis. Results of CPDDevice and TTFCDevice were used for categorizing these variables in the same way as corresponding FTND items. Categorizing PCDevice and TSTDevice is done in the same way as PCSurvey and TSTSurvey. The association between self-reported smoking habits and topography variables measured using the CReSS Pocket devices was investigated by calculating Spearman’s correlation coefficient (ρ). We also tested the reliability of the self-reported smoking habit parameters by calculating Cronbach’s α and Cohen’s Kappa. The median difference between the corresponding variables measured by the survey and topography device was tested thorough Wilcoxon signed-rank test. All statistical analysis was conducted using IBM® SPSS® Statistics version 25 (IBM Company, Armonk, NY, USA) with a significance level set at 0.05.
Results and Discussion
Results of machine-determined smoking topography and self-report smoking habit survey
Results of machine-determined smoking topography and self-reported smoking habits are presented in Table 2. The ratio of the number of male participants to female participants is around 6.1, which is close to the ratio of male smokers to female smokers on a nationwide scale [8]. Considering the location where we conducted our study and the population density of South Korea, most of the participants were residents of Seoul.
The average FTND score of the participants is calculated to be 3.13, which indicates a low nicotine dependency. More than 70% of the participants were evaluated to have low or very low nicotine dependency and only 4% of the participants had an FTND score of more than 8. The TTFCFTND for more than 50% of the participants was 30 minutes after waking up. The average CPD determined by the smoking topography device (CPDDevice) is close to the CPDSurvey, which is calculated based on the results of the questionnaire items for the average number of cigarettes smoked during weekdays and weekends separately. The difference between the average CPDWeekdays and CPDWeekends is only one cigarette. The averages of PCDevice and TSTDevice were 20.4 and around 3 minutes, respectively. According to the results of the self-report smoking habit survey, the majority of the participants declared that they try to smoke their cigarette with less than 14 puffs and within 1–1.5 minutes. Eleven subjects failed to report their wake-up time and were therefore excluded from the TTFCDevice analysis. Under this circumstance, the average of TTFCDevice was approximately 79 minutes.
Association between variables measured using the survey and the smoking topography device
Table 3 shows the results of the association analysis between the variables measured through the self-report smoking habit survey and those measured using the CReSS Pocket device. Results indicate a distinct positive and statistically significant association between CPDSurvey and CPDDevice (ρ=0.571, p<0.001). CPDSurvey also has a weak, negative, and statistically insignificant correlation with total smoking time. These results are consistent with the study of Yang et al. [7].
Results also yield that the TTFCFTND and TTFCDevice have a strong negative and statistically significant correlation (ρ = −0.587, p<0.001). The negative sign of the correlation coefficient is mainly because of the scoring method of FTND [17]. A higher measured TTFCDevice indicates a lower TTFCFTND score, which means lower nicotine dependency. Results also indicate that CPDDevice, TTFCDevice, and TSVDevice have distinct positive and statistically significant correlations with FTND scores. Furthermore, TSVDevice has a weak positive association with smoke inhalation depth, which is significant at the 10% significance level.
Correlations between PCSurvey and TSTSurvey with the corresponding machine-determined variables, puff count and total smoking time, are positive but are neither strong nor statistically significant. The correlation between PCSurvey and machine-determined puff count in our study is lower than the one reported by Shahab et al. [14] which was between 0.2–0.4.
Reliability of variables measured by the survey compared to results obtained using the smoking topography device
The Cronbach’s α was calculated for variables measured by the self-report smoking habit survey against the corresponding ones measured by the CReSS Pocket device. Cronbach’s α for CPDSurvey and CPDDevice was calculated to be 0.623, indicating a relatively high reliability of the average number of daily smoked cigarettes investigated by the self-report smoking habit survey. Similarly, the Cronbach’s α for TTFCFTND and TTFCDevice was 0.754. Accordingly, it may be possible to rely on surveys such as FTND that are designed based on the self-reported daily smoked cigarettes for clinical and tobacco smoke risk assessment exposures [7, 15, 17]. Cronbach’s α values calculated for PCSurvey and TSTSurvey against machine-determined puff count and total smoking time were 0.053 and −0.020, respectively. The positive value of Cronbach’s α for puff count is consistent with the results presented by Shahab et al. [14].
The results of inter-rater reliability evaluation between smoking habit variables obtained using the survey with the corresponding ones measured by topography device and calculated using Cohen’s Kappa value were consistent with the results of Cronbach’s α. In particular, the Kappa value for agreement between TTFCFTND and TTFCDevice was calculated to be 0.298, which was statistically significant (p=0.001). For TTFCFTND and TTFCDevice, the Kappa value was 0.226 (p<0.001). This is in contrast with the Kappa values calculated for PCSurvey and TSTSurvey against PCDevice and TSTDevice were −0.041 (p=0.252) and 0.009 (p=0.791), respectively, indicating very weak and statistically insignificant inter-rater reliability.
Comparison of results based on multiple answers in the self-report smoking habit survey
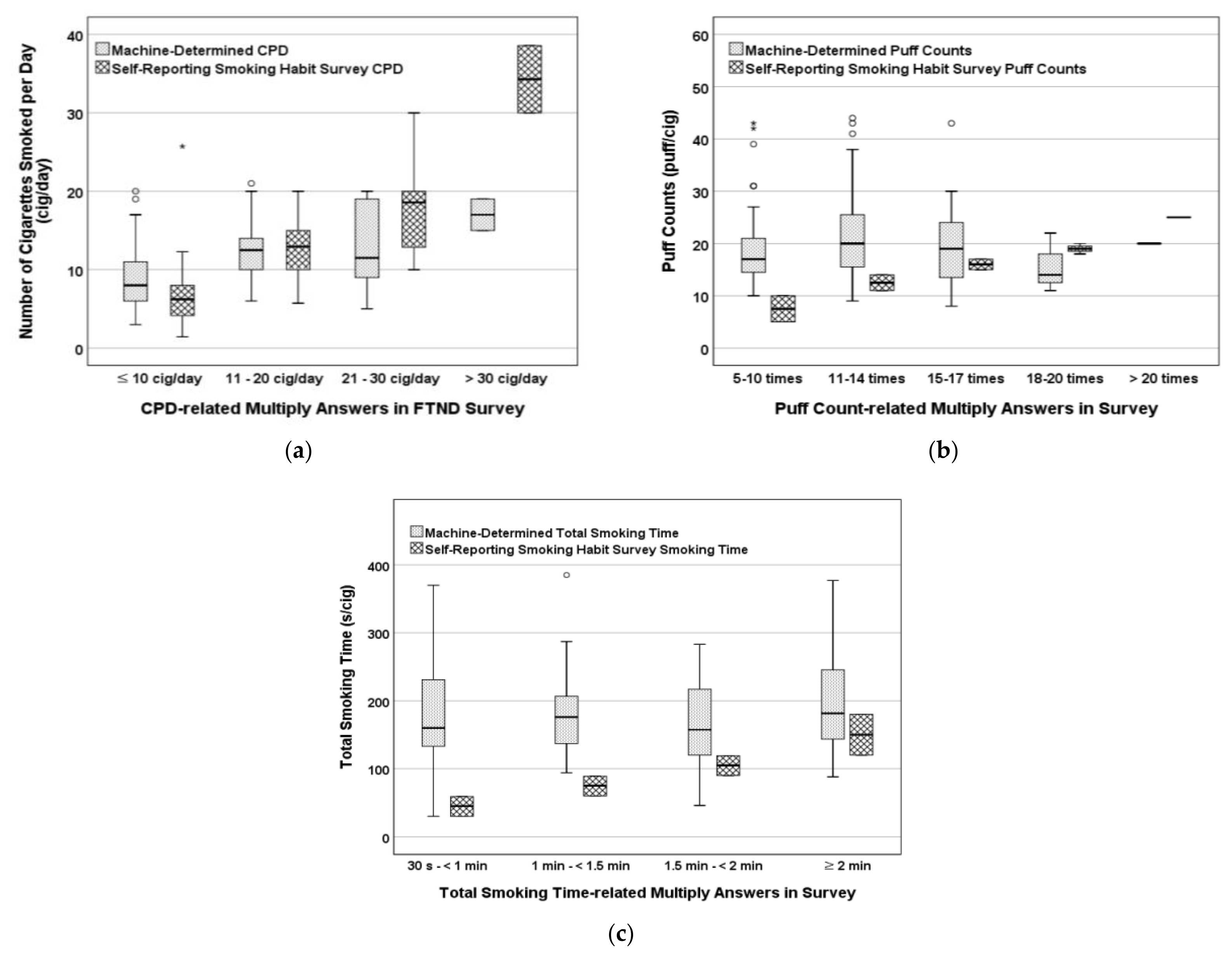
Figure 1 presents the comparison of the results for the number of cigarettes smoked per day, puff counts, and total smoking time measured using the CReSS Pocket device and the self-report smoking habit survey. Results indicate that majority of the smokers have relatively accurate knowledge of the average number of cigarettes they smoke per day.
Nevertheless, two smokers who declared that they smoke more than 30 cigarettes per day in the self-report survey have over-reported. The Wilcoxon signed-rank test results indicated that there was no statistically significant difference between the median of CPDSurvey and CPDDevice measurements (z= −1.002, p=0.316, r=0.100). In contrast, there was a statistically significant difference between the puff counts (z = −7.639, p < 0.001, r = 0.764) and total smoking time (z= −7.928, p<0.001, r=0.793), with a relatively large effect size.
Regarding puff count, the Wilcoxon signed-rank test result shows that 85% of the smokers underestimate the puff number per cigarette. This finding is consistent with the results of Pulcu [16] with English smokers under-reporting puff numbers in a self-report survey. Similarly, 86% of smokers under-reported the total smoking time in the self-report survey. This indicates that the majority of smokers are exposed to cigarette smoke for a longer period than they think they are. In this regard, it is essential to rely on the results that are obtained using smoking topography measurement devices to have a more realistic understanding of cigarette smokers’ exposure to tobacco smoke.
Since about 10% of the subjects failed to provide their wake-up time, we could not calculate the TTFCDevice for them. Accordingly, because the Wilcoxon signed-rank test results are heavily related to the number of available data, we decided to exclude running the test between the TTFCFTND and TTFCDevice.
Study limitations
This study should be considered with several limitations that are primarily due to limited funds and resources. The number of participants is relatively small compared to the nationwide population of South Korea and the majority of the participants were not heavy smokers. Due to the social limitations during the COVID19 pandemic, it was challenging to execute the investigation to involve more subjects. Moreover, the number of female smokers who volunteered to participate in this study was relatively lower than male smokers owing to cultural challenges. Also, considering the location of the venue where we conducted our study, we could not gather many subjects from provinces of South Korea that are of considerable distance from Seoul. Finally, since 11 subjects decided not to report their wake-up time, there were challenges in analyzing the TTFCDevice for the whole study community.
Nevertheless, we believe that these limitations may not have a significant effect on the results, which are consistent with those obtained by several prior studies such as Shahab et al. [14] in 2008 and Pulcu [16] in 2016, which were conducted with a similar number of subjects as the present study [14,16]. It is also worth noting that the ratio of the number of male smokers to female smokers in this study is close to the ratio of male smokers to female smokers on the nationwide scale.
Conclusions
In this study, we have examined different smoking habit variables using a self-report survey and smoking topography measurement device for a group of Korean smokers. We then compared the results and investigated their association and reliability with the results obtained from the smoking topography measurement device. Our results demonstrate that Korean smokers have a relatively realistic understanding of the average number of cigarettes they smoke daily and the time to their first cigarette of the day. Nonetheless, they under-report their puff numbers and total smoking time, which are key elements in measuring exposure to tobacco smoke. Underestimating these key variables can significantly lead to underestimation of risks of exposure to tobacco smoke. Accordingly, it is recommended not to rely on self-report surveys for smoking topography measurements. Instead, using surveys that are based on measuring the number of cigarettes smoked daily such as FTND, is more reliable for clinical applications, risk assessment procedures, and in designing applicable smoking cessation programs. Accordingly, we recommend that the national organizations running nationwide health investigation programs such as the Korea National Health and Nutrition Examination Survey (KNHANES) to include both FTND and topography measurements for active smokers in their survey programs.